ABORTION
- Mar 11
- 5 min read
🔶 DEFINITION : An expulsion or extraction on embryo or fetus before the 20 week of gestation weight less than 500 gm when it is not capable to independence survive.
🔶 CAUSES
1.Chromosomal abnormalities
In about 50% cases of abortion, chromosomal abnormalities found in the fetus are responsible for it.These include
Trisomy
Polyploidy
Monosomy
Other abnormalities
2. Anatomical abnormalities
Incompetent cervix - This is the most common cause of abortion during second trimester.
Congenital malformations of the uterus.
Fibroid
3.Infection
Viral infections such as rubella, herpes simplex, cytomegalovirus, HIV etc.
Bacterial infections such as brucella, chlamydia, spirochaetes etc.
Parasitic infections such as toxoplasmosis, malaria etc.
4.Endocrinal factors
Luteal Phase Defect (LPD).
Hyper or hypo secretion of thyroid gland (Hyperthyroidism or hypothyroidism).
Deficient secretion of progesterone hormone from the corpus luteum.
5.Maternal diseases
Diabetes mellitus
Heart disease
Chronic nephritis
Malnutrition and anaemia
🔶 CLASSIFICATION OF ABORTION
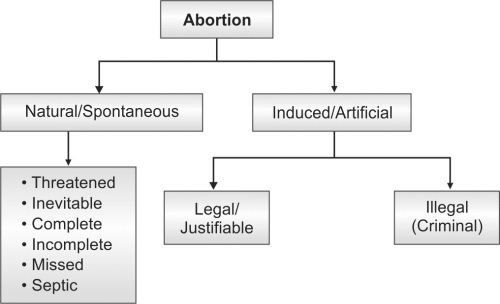
1️⃣ INCOMPLETE ABORTION
The type of abortion in which during the process of abortion, some products of conception expel out the uterine cavity whereas some remain inside, is known as incomplete e abortion.
🔸CLINICAL MANIFESTATIONS
Passage of clots or pieces of tissue through the vagina.
Vaginal bleeding (moderate to heavy).
Colicky pain in lower abdomen (cramp-like pain).
Cervical dilatation (cervix is open).
Signs of shock due to bleeding – hypotension, tachycardia, dizziness, restlessness.
Uterus smaller than the period of amenorrhoea on obstetric examination.
🔸MANAGEMENT
Check the patient’s vital signs, general condition, and severity of bleeding.
Control bleeding
Give uterotonic injections such as Ergometrine or Syntometrine to reduce excessive bleeding.
Anti-shock treatment
Start treatment for shock by giving IV fluids (Ringer Lactate) and blood transfusion if necessary.
Pain management
Give analgesic drugs to relieve abdominal pain.
Evacuation of uterus
Perform uterine evacuation to remove the remaining products of conception.
2️⃣ COMPLETE ABORTION
The type of abortion in which all the products of it conception are expelled out from the uterus, is known as complete abortion
🔸CLINICAL MANIFESTATIONS
History of passage of clots and pieces of tissue through the vagina.
Vaginal bleeding decreases after expulsion of all products of conception.
Lower abdominal pain reduces or stops after abortion is complete.
Cervix becomes closed on examination.
Uterus becomes smaller than the period of amenorrhoea.
Patient’s general condition improves and signs of shock are usually absent.
🔸MANAGEMENT
Confirm diagnosis by ultrasound if the case is doubtful.
Uterine curettage may be done using aseptic technique if required.
Anti-shock treatment – give IV fluids and blood transfusion if necessary.
Provide psychological support because the woman may be upset after pregnancy loss.
If the woman is Rh-negative, give Rho(D) Immune Globulin injection as prescribed.
Maintain proper nutrition and general care of the woman.
3️⃣ THREATENED ABORTION
The type of abortion where the process of abortion has started but has not affected the fetus to a state from where recovery is not possible, is known as threatened abortion. In these types of abortions, in about 75% of cases, the pregnancy continues normally.
🔸CLINICAL MANIFESTATIONS
Vaginal bleeding - It is usually scanty and bright red coloured. In some cases, it may be heavy.
Colicky pain in lower abdomen.
Backache
General health status of the woman is stable.
As the fetus is alive so in most of cases pregnancy continues normally.
🔸DIAGNOSIS
Routine blood and urine investigations.
Ultrasonography.
Estimation of serum hCG level.
Estimation of serum progesterone level Serum progesterone level more than 25 mg /ml is the indicative of viable fetus.
🔸INTERNATIONAL EXAMINATION
Size of the uterus is in accordance with the period of gestation.
Cervical os is generally closed or may be patulous.
Ultrasonography examination reveals a viable pregnancy.
🔸 POSSIBLE OUTCOME
Pregnancy continues normally if bleeding stops and proper care is taken.
Spontaneous abortion (miscarriage) may occur if the condition worsens.
🔸 MANAGEMENT
Complete bed rest is advised.
Avoid heavy work, travel, and sexual intercourse.
Sedatives and analgesics may be given if required.
Hormonal therapy such as progesterone may be prescribed by the doctor.
Regular monitoring and follow-up with ultrasound.
Provide emotional support to the patient.
4️⃣ INEVITABLE ABORTION
it is an abnormal condition occurring before 20th completed weeks of pregnancy characterized by profuse vaginal bleeding and dilated cervix in which expulsion of the products of the conception from the uterine cavity is certain.
*🔸 CLINICAL MANIFESTATIONS
Profuse vaginal bleeding.
A Presence of colicky pain in the lower abdomen - It is of severe type.
A Due to heavy vaginal bleeding, clinical features of shock may appear such as hypotension, tachycardia, dizziness, restlessness etc.
MANAGEMENT
Assess vital signs, general health status and severity of clinical manifestations.
Reassure the woman and provide psychological support.
To control bleeding, administer inj. Ergometrine 0.5mg or Methargin 0.2mg as per doctor's prescription.
Provide anti shock treatment. Start IV line and administer fluid such as RL drip. Cross matched blood should also be transfused if required.
Advise the woman and her family members to preserve the perineal pads and other discharges through the vagina for examination.
Administer analgesics to relieve pain.
Administer prophylactic antibiotics to reduce risk of secondary infections.
Evacuation of the uterus.
5️⃣ MISSED ABORTION
It is an abnormal condition in which fetus has died but is retained inside the uterus.
Missed Abortion is also known as silent miscarriage
🔸 CLINICAL MANIFESTATIONS
Brownish vaginal discharge – Light brown discharge may occur from the vagina.
Pain absent – Usually there is no abdominal pain.
Pregnancy symptoms decrease – Morning sickness and breast tenderness reduce or disappear.
No weight gain – The woman does not gain weight as expected in pregnancy.
Uterus smaller than gestational age – The uterus is smaller than the expected size of pregnancy.
Uterus feels hard – On examination the uterus feels firm instead of soft.
Pregnancy test negative – Pregnancy test may become negative after fetal death.
Fetal heart sound absent – The fetal heartbeat is not heard though it was heard earlier.
Breast changes regress – Breast enlargement and tenderness decrease.
No fetal movements – The mother does not feel fetal movements.
🔸 MANAGEMENT
Confirm diagnosis by ultrasound and obstetrical examination.
Evacuation of the uterus to remove retained products of conception (e.g., Dilation and Curettage).
Induction of uterine contractions using drugs such as Misoprostol.
Monitor vital signs and bleeding regularly.
Give antibiotics to prevent infection if required.
Provide emotional and psychological support to the woman.
If the woman is Rh-negative, give Rho(D) Immune Globulin as prescribed.
6️⃣SEPTIC ABORTION
Infected abortion characterized by fever, tachycardia, pain abdomen etc. is known as septic abortion. In other words we can say that infection of the products of conception is known as septic abortion.
Septic Abortion commonly occurs following unsafe induced abortion
🔸 CAUSES
Streptococci
Staphylococci
E.Coli
Clostridium welchii
Clostridium tetani
Klebsiella
Pseudomonas
Chalmydia
🔸 RISK FACTOR
Unsafe abortion
If the woman is suffering from Sexually Transmitted Diseases (STDs).
If the fetal membranes surrounding the fetus have ruptured.
Insertion of sticks, chemicals, pastes or soaps into the pregnant uterus
🔸 CLINICAL MANIFESTATIONS
High grade fever (Usually more than 1010F).
Tachycardia (Increased pulse rate).
Presence of foul smelling discharges through the vagina.
Severe pain in abdomen or cramping.
Backache
In serious condition, following features of septic shock may appear -
Hypotension
Tachycardia
Hypothermia
Decreased urinary output
Restlessness and dizziness
Difficulty in breathing
🔸 MANAGEMENT
Start broad-spectrum antibiotics immediately.
Give IV fluids and treat shock if present.
Evacuate the uterus after controlling infection.
Blood transfusion if severe bleeding occurs.
Monitor vital signs regularly.
Comments