Pancreatitis
- Jul 28, 2023
- 4 min read
Updated: Apr 26, 2025
Pancreatitis is inflammation of the pancreas, which can either be acute (sudden and severe) or chronic (ongoing). The pancreas is a gland that secretes both digestive enzymes and important hormones.

Types
Acute pancreatitis
Chronic pancreatitis
Hereditary pancreatitis.
Acute pancreatitis
Acute pancreatitis is a sudden inflammation of the pancreas. The pancreas is a small organ located behind the stomach that produces enzymes that help with digestion. When the pancreas becomes inflamed, these enzymes can start to digest the pancreas itself, which can cause pain, swelling.
Chronic pancreatitis
a progressive inflammatory disorder that leads to irreversible destruction of exocrine and endocrine pancreatic parenchyma caused by atrophy and/ or replacement with fibrotic tissue.
Causes
Remember💡
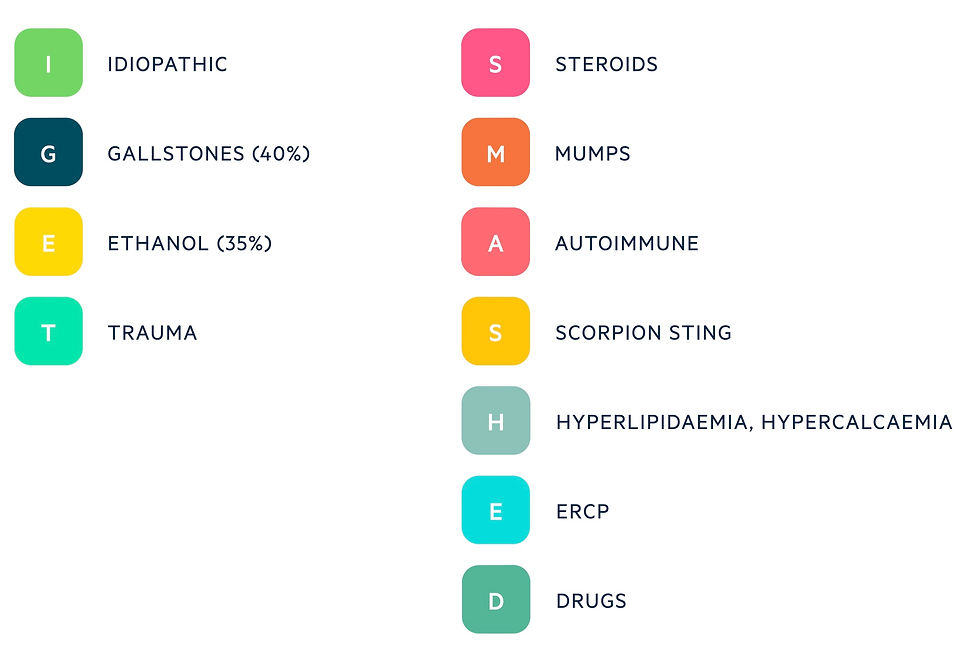
"I GET SMASHED MEDVIPS"
I- Idiopathic
G- Gall stone(Cholelithiasis)
E- Ethanol
T- Trauma
S- Steroids
M- Mumps
A- Auto Immune disease like SLE (systematic lupus erythomas)
S- Scorpion 🦂 or snake 🐍 posioning
H- Hypercalcemia/ Hyperlipidemia
E - ERCP ( Endoscopic Retrograde Choleangio Pancreatography)
D- Drugs
M - Metronidazole
E- Estrogen
D- Didasonine
V- Valporate
I- Isoniazide
P- Pentamide
S - Sulfonamide
Less common causes of pancreatitis include:
Infections, such as viruses.
Autoimmune disease (autoimmune pancreatitis).
Inherited gene mutations (hereditary pancreatitis).
Complications of cystic fibrosis.
High blood triglyceride levels (hypertriglyceridemia).
High blood calcium levels (hypercalcemia).
Ischemia (reduced blood supply).
Cancer.
Traumatic injury to your pancreas.
Certain medications that irritate the pancreas.
Sign and Symptoms
Symptoms
Abdominal pain (may radiate to the back)
Nausea
Vomiting
Anorexia
Diarrhoea
Steatorrhea ( Grady /fatty stool float on water )
Indegestion
Bloting
Weight loss
Flatulence
Polyuria
Polydipsia( increased thirst)
Signs
Abdominal tenderness
Abdominal distention
Tachycardia
Tachypnea
Pyrexia
Cullen’s sign: peri-umbilical bruising (first described in ruptured ectopic pregnancy)
Grey-Turner’s sign: flank bruising
Complications
Necrosis and infection
Pancreatic pseudocysts
Exocrine pancreatic insufficiency (EPI)
malabsorption / malnutrition
Hypoglycemia
hyperglycemia
Type 1 diabetes mellitus
Pancreatic cancer
Duodenal obstruction
Biliary obstruction
Diagnosis
History collection
Physical examination
CBC
Urea & electrolytes
Lipase/ amylase/ trypsin
Liver function tests
Lipid profile
Bone profile
Magnesium
HbA1c
Vitamin D
Glucose test (to see whether your pancreas is still producing insulin effectively).
Stool elastase test (to see if your pancreas is making enough digestive enzymes).
Fecal fat analysis (to test for excess fat in your poop, a sign of fat malabsorption).
Arterial blood gas (assess oxygenation and acid-base, pO2 is also used for scoring acute pancreatitis)
Imaging
CT: enables confirmation of diagnosis and to assess for possible cause
MRI/MRCP
X-ray
Endoscopy
Special test
Bone mineral density: at risk of osteoporosis
Genetic testing: consider if idiopathic chronic pancreatitis or strong family history
IgG subsets: specifically for autoimmune pancreatitis
Glasgow score
The Glasgow score, completed in the first 48hrs, helps to assess the severity of acute pancreatitis.

Treatment
General management
General management consists of analgesia, appropriate fluids and nutritional support.
The majority of cases of acute pancreatitis are treated with supportive measures. This normally includes:
IV fluids
Analgesia
Nutritional support

General Medical Management of Chronic Pancreatitis:
1. Pain Management:
- Non-opioid analgesics: Acetaminophen (Paracetamol) is the first-line for mild to moderate pain.
- Opioids may be used for severe pain but should be monitored closely due to the risk of dependence.
- NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) are generally avoided due to their potential to worsen pancreatitis.
2. Enzyme Replacement Therapy:
- Pancreatic enzyme replacement therapy (PERT) with pancreatic enzyme supplements (lipase, amylase, protease) to aid digestion.
- Dose: Dosage varies based on the severity of malabsorption and the individual's needs. Commonly, a high lipase dose (e.g., 25,000-40,000 units) is taken with meals, and half the dose is taken with snacks.
3. Nutritional Support:
- Work with a dietitian to plan a low-fat, high-protein, and nutrient-rich diet.
- Smaller, frequent meals may be better tolerated than large meals.
- Fat-soluble vitamin supplementation (A, D, E, and K) may be necessary due to malabsorption.
4. Management of Diabetes:
- Control blood glucose levels with lifestyle modifications and antidiabetic medications as prescribed by a healthcare provider.
5. Management of Complications:
- Pseudocysts: Small pseudocysts may resolve on their own, but larger or symptomatic ones may require drainage or endoscopic intervention.
- Bile duct obstruction: Treatment may involve stenting or surgery to relieve obstruction.
- Malabsorption: Monitor for fat-soluble vitamin deficiencies and manage with supplementation.
6. Lifestyle Modifications:
- Avoid alcohol consumption, as it can exacerbate pancreatitis.
- Stop smoking, as it increases the risk of pancreatitis and disease progression.
7. Treatment of Underlying Causes:
- Address any identifiable causes of chronic pancreatitis, such as gallstones or autoimmune conditions.
Surgical management
1. Pancreatic Necrosectomy: Surgical removal of necrotic (dead) tissue from the pancreas to prevent infection and improve organ function.
2. Pancreatic Abscess Drainage: A procedure to drain fluid-filled abscesses that have developed in the pancreas.
3. Pancreatic Pseudocyst Drainage: Drainage of fluid collections (pseudocysts) that have formed around the pancreas.
4. Pancreaticoduodenectomy (Whipple Procedure): Surgical removal of the head of the pancreas, part of the small intestine (duodenum), gallbladder, and bile ducts for cases of severe or malignant pancreatitis.
5. Distal Pancreatectomy: Removal of the tail and body of the pancreas, leaving the head intact.
6. Total Pancreatectomy: Complete removal of the pancreas, often considered in severe cases or if other treatments fail.
7. Pancreatic Stent Placement: Insertion of a stent to open blocked pancreatic ducts and improve drainage.
8. Gastric Bypass Surgery: In some cases, gastric bypass surgery may be performed to bypass the pancreas, which can help manage symptoms of chronic pancreatitis.
9. Pancreatic Islet Cell Transplantation: A specialized procedure where isolated islet cells from a donor pancreas are transplanted into a patient with chronic pancreatitis to improve insulin production.
Please note that the specific surgical approach will depend on the severity and type of pancreatitis, as well as the patient's overall health condition.
Comments